 English
English  Ελληνικά
Ελληνικά 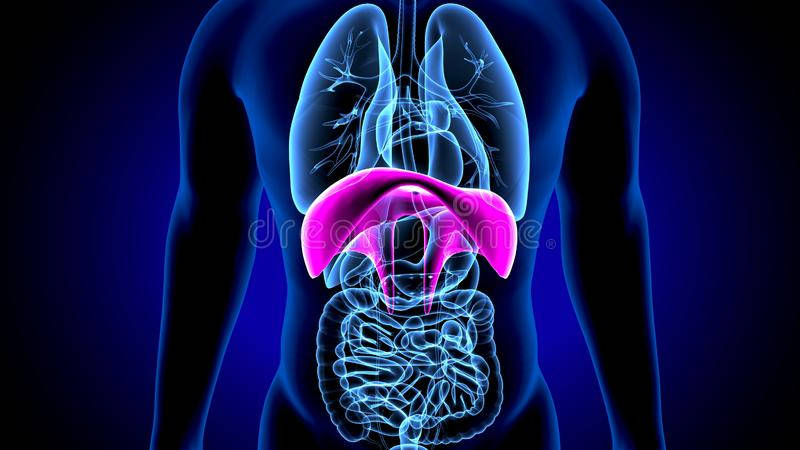
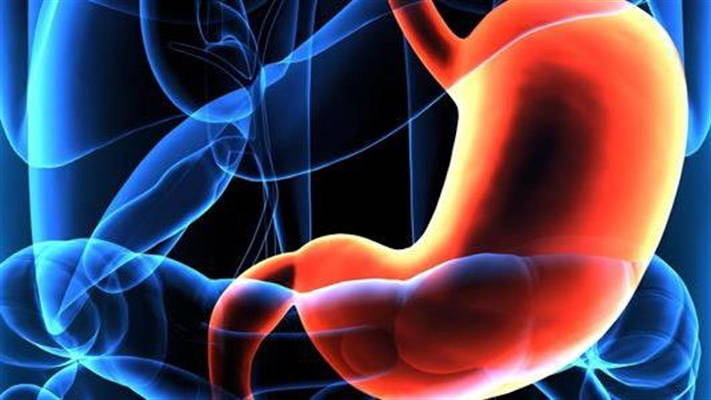
The thoracic cavity is separated from the abdominal cavity by a strong muscular lining called the diaphragm. The role of the diaphragm, apart from being separating and protective, is also functional because it contributes to respiration. The diaphragm also has an opening (esophageal foramen) through which the esophagus passes from the thorax to the abdomen and is conjugated with the stomach.
The term diaphragmatic hernia is used to describe the enlargement of the esophageal foramen and the displacement of intra-abdominal viscera into the mediastinum.
Depending on the part of the stomach that prolapses the diaphragmatic hernia is classified into:
- Lapsive or type I where only the gastroesophageal junction is displaced intrathoracically.
- Paraesophageal or type II where the stomach fornix prolapses into the thorax and the gastroesophageal junction remains in place.
- Mixed or type III which is a combination of the two
Paraesophageal or type IV where the esophageal foramen is lanced so much that besides the stomach other organs such as the small or large intestine also protrude through it to the mediastinum. Symptoms of intestinal obstruction or stomach convolution may occur.
Predisposing risk factors are:
- Advanced age associated with muscle weakness and loss of tissue elasticity.
- Obesity
- Pregnancy
- Ascetes
- Increased intra-abdominal pressure as with chronic cough, constipation and weight lifting.
Most patients with diaphragmatic hernia are asymptomatic. In the rest it causes symptoms of gastroesophageal reflux. Gastroesophageal reflux is the reflux of stomach contents (gastric fluid, food) to the esophagus. The most common symptoms are heartburn, reductions, difficulty swallowing, nausea and eructations (belchings). In addition to the symptoms, gastroesophageal reflux can cause inflammation of the esophagus (esophagitis) which in turn can cause lesions of the esophageal mucosa (Barret esophagus) which is a precancerous condition. There may also be non esophageal-related symptoms such as chronic cough, laryngitis, pharyngitis, hoarseness and aspiration pneumonia.
The diagnosis is made by:
- Gastroscopy
- Special radiological examination (esophagus and stomach passage with gastrographin)
- Pechametry (24-hour measurement of pH inside the esophagus to reveal gastroesophageal reflux)
- Manometry (measurement of the pressure of the esophageal sphincter to separate from another condition called esophageal achalasia)
- In rare cases, a CT scan is required
Gastroesophageal reflux caused by diaphragmatic hernia can be treated depending on the patient either conservatively or surgically.
Conservative treatment includes:
- Taking medicines that limit the production or acidity of gastric fluid
- Avoiding foods that aggravate gastroesophageal reflux (fried, chocolate, alcoholic)
- Weight loss
- Avoiding meals before going to bed
- Not recumbent position during sleep
In case of failure of conservative treatment, the diaphragmatic hernia is treated with open, laparoscopic or robotic surgery. The surgeon narrows the diaphragmatic foramen with sutures during surgery. In case the foramen is too big, the sutures are strengthened by placing a plexus. The stomach is then restored into the venter and part of it is wrapped around it (gastric vault plication). Vault plication can be done either by 360 degrees (Nissen) or by 270 degrees (Toupet).
The advantages of laparoscopic and robotic surgery over open surgery are:
• Less pain after surgery
• Faster discharge from hospital, faster recovery and return to daily activities and work
• Reduction of immediate and distant complications.
The surgical treatment has very good results.